Browse through our Journals...
TONGUE INTRAMUSCULAR LIPOMA
Roberta Leitão FIGUEIREDO1, Cássio Roberto Rocha dos SANTOS1, Nádia Lages LIMA2, Flaviana Dornela VERLI2, João Luiz de MIRANDA2, Sandra Aparecida MARINHO1,2*
1Oral Medicine Clinic, Dentistry Course, Federal University of Jequitinhonha and Mucuri Valleys (UFVJM), Diamantina, MG, Brazil
2 Pathology Laboratory, Department of Basic Sciences, UFVJM, Diamantina, MG, Brazil
*Corresponding author
Sandra Aparecida Marinho
Address for reprints:
Laboratório de Patologia-UFVJM
Rua da Glória, 187, Prédio 2, Sala 22, Campus I, CEP: 39100-000, Diamantina, MG, Brazil
ABSTRACT
Intramuscular lipoma is a benign tumor that rarely occurs in the oral cavity, with few cases described in the literature. This paper reports a clinical case of intramuscular lipoma on the tongue of a 53-year-old patient.
Keywords: lipoma, tongue, intramuscular
INTRODUCTION
Lipoma is a benign mesenchymal fat cell tumor that is common in the trunk and proximal portion of the limbs, but rarely occurs in the mouth and maxillofacial region. Clinically, lipoma is an asymptomatic nodular mass with slow growth and a yellowish color when superficial and with coloration similar to normal mucosa when more deeply located (Akbulut et al, 2005; Nishida et al, 2007). Histologically, lipoma is indistinguishable from normal fat tissue, but its lipids are unavailable for metabolism (Epivatianos et al, 2000).
In the oral cavity, lipoma occurs more frequently in the buccal and vestibular mucosa, with the tongue, floor of the mouth and lips less commonly affected. Diverse variants of lipoma are described, such as angiolipoma, spindle cell lipoma, pleomorphic lipoma and intramuscular or infiltrating lipoma (Akbulut et al, 2005; Epivatianos et al, 2000; Thomas et al, 2002; Scolozzi et al, 2003;). Intramuscular lipoma is a rather rare pathology in the oral cavity, with few cases reported in the literature [4,6] (Thomas et al, 2002; Keskin et al, 2002). Intramuscular lipoma has a tendency toward recurrence following incomplete excision (Thomas et al, 2002; Scolozzi et al, 2003) due to the fact that it does not have a well-defined capsule [1] (Akbulut et al, 2005).
This paper presents a clinical case of intramuscular lipoma on the tongue, describing the clinical and histopathological characteristics.
CASE REPORT
A 53-year-old male patient, melanoderm, was referred to the Stomatology Clinic of the Federal University of Jequitinhonha and Mucuri Valleys, UFVJM (Brazil) by a private dentist. The patient history revealed the use of diazepam (10 mg), current smoking habit and a past history of alcoholism. The oral exam revealed a painless, sessile, nodular lesion with the color of normal mucosa, measuring approximately 1 cm on the right lateral edge of the tongue near the premolar region. The clinical diagnosis was fibroma and an excisional biopsy was performed. The histopathological exam revealed the surface of the lesion to be covered with hyperkeratinized, hyperplastic, stratified, squamous epithelium originating from the oral mucosa. Below this, there was a mass of mature fat tissue intercalated with atrophied skeletal muscle fibers. Surrounding this tissue mass, there was dense fibrous conjunctive tissue forming a fibrous capsule. The histopathological findings confirmed the diagnosis of intramuscular lipoma and the patient is currently in follow up.

Figure 1: Nodular lesion on right lateral edge of tongue
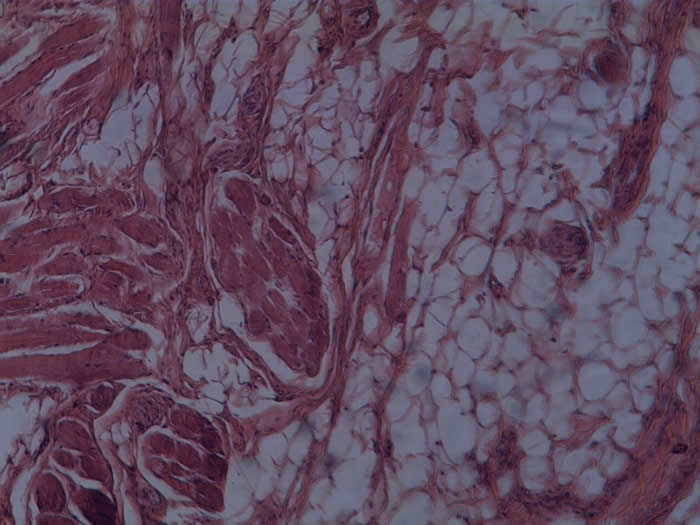
Figure 2: Fat tissue amid normal muscle tissue
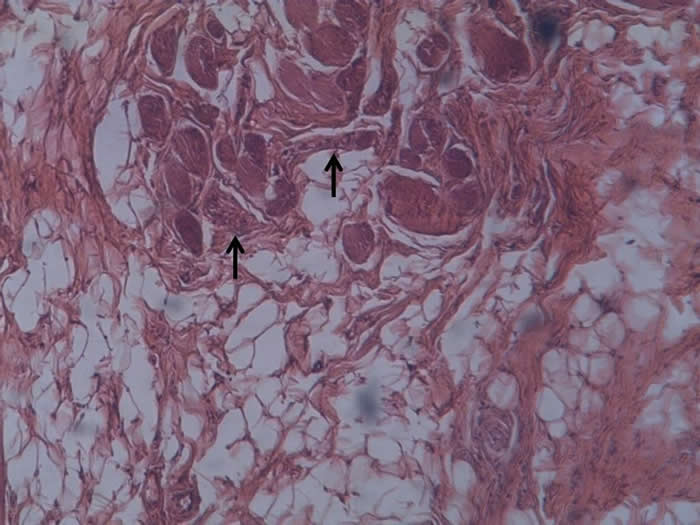
Figure 3: Fat tissue with mature fat cells with nuclei located peripherally and intertwining muscle tissue with some degree of atrophy (arrows)
DISCUSSION
Intramuscular lipoma is a rather rare tumor (Thomas et al, 2002; Keskin et al, 2002;) characterized by invasion into muscle tissue or growth between muscle fibers and is sometimes denominated infiltrating lipoma (Salvatore et al, 2003). Nishida et al (2007) carried out a retrospective study on 40 patients with intramuscular lipoma and found that the lesions most commonly occurred on the thigh. Only five (12.5%) of the lipomas were encapsulated. However, the authors did not report any cases of oral intramuscular lipoma and only one case on the neck.
Akbulut et al (2005) carried out a review of 13 cases of intramuscular lipoma on the tongue, five of which occurred in men and eight occurred in women, with patient age ranging from 37 to 81 years (mean: 60.6 years). The patient of the present case report falls within this age range (53 years). Epivatianos et al (2000) found no differences between genders in a literature review of 10 cases of intramuscular lipoma. In their own study, the authors describe 13 cases of lipoma, only two of which were intramuscular. According to the authors, in the oral cavity, there is a slight predilection for the tongue due to the close contact between fat and muscle tissue. The authors also state that there is no consensus in the literature on whether oral intramuscular lipoma is actually a pathological entity or whether it is a true lipoma entrapped in muscle fibers. Fregnani et al (2003) analyzed 46 cases of lipoma, six of which were located on the tongue and only two of these were intramuscular; the remaining intramuscular lipomas were found on the buccal mucosa and floor of the mouth. Freitas et al (2009) analyzed 26 cases of oral lipoma and found that only two were diagnosed as intramuscular, both of which were located on the tongue. Furlong et al (2004) analyzed 124 cases of lipoma of the head and neck and found that 15 occurred on the tongue.
The clinical diagnosis of the case reported here was fibroma, with focal fibrous hyperplasia as the diagnostic hypothesis, which is in agreement with the diagnostic hypotheses described by Tateyama et al (2005). According to the authors, in cases in which the lesion has the color of the adjacent mucosa, the hypotheses of fibroma and hyperplasia are more plausible than lipoma. As the patient in the present case was alcoholic, the hypothesis was raised of traumatic injury as a consequence of a fall or bite on the tongue. However, the patient did not report any such occurrence. According to Moore et al (2001), the differential diagnosis of lipoma on the tongue should include schwannoma, cyst and adenoma of the minor salivary glands. In the case describe here, the hypothesis of this lesion was not originally raised due to the rarity of its location in the oral cavity and the absence of typical clinical characteristics of lipoma.
The patient had no pain. The only symptom was a discreet increase in volume on the tongue. Nishida et al (2007) report the most common symptoms of intramuscular lipoma to be an asymptomatic mass (24 lesions) and swelling with no palpable mass (13 lesions); only three lesions were painful.
The size of the lesion in the present case (1 cm) is in agreement with a survey carried out by Fregnani et al (2003) involving 46 cases of lipoma ranging in size from 0.3 to 5 cm; among the lesions, only 8.6% were intramuscular. Keskin et al (2002) report one case of multiple lesions on the tongue, the largest of which was 1 cm in diameter. Colella et al (2009) report a case of giant intramuscular lipoma on the tongue, with a diameter of 10 cm and 30 years of evolution, which hindered the speech and deglutition of the 75-year-old patient. Kacker and Taskin (1996) report a case of a 6-cm intramuscular lipoma on the tongue that hindered the mastication and deglutition of the patient. Matsumoto et al (1999) report that intramuscular lipoma is likely benign when the diameter is less than 3 cm, without taking the regularity of its margins and homogeneity into consideration. Furlong et al (2004) analyzed 125 cases of lipoma of the head and neck and report a mean size of 2.2 cm; 23 were intramuscular and 15 were located on the tongue, eight of which were intramuscular.
The histopathological findings in the present case were compatible with intramuscular lipoma, with the presence of mature fat cells infiltrating the muscle fibers. The muscle fibers exhibited different degrees of atrophy, with no cellular atypia, mitotic activity, multinucleated cells, inflammation or necrosis (Akbulut et al, 2005; Thomas et al 2002; Keskin et al, 2002; Fregnani et al,2003; Freitas et al, 2009; Colella et al, 2004). There was also an absence of lipoblast proliferation (Akbulut et al, 2005; Collela et al, 2009). Moreover, the fat cells infiltrating the muscle fibers were all mature and uniform in shape and size (Colella et al, 2009). The nuclei of the lipocytes were small, flattened and peripherally located (Nishida et al, 2007). It should be stressed that intramuscular lipoma may also give a false-positive diagnosis of liposarcoma, but the absence of pleomorphism and cellular hyperchromatism, along with the low mitotic activity, supports the diagnosis of infiltrating lipoma (Nishida et al, 2007; Epivatianos et al, 2000; Fregnani et al, 2003). Thus, pathologists should be quite discerning in the evaluation of such lesions. The presence of occasional lipoblasts in an infiltrating tumor made predominantly of mature fat cells, along with the absence of mitotic figures and pleomorphism, characterizes the diagnosis of typical intramuscular lipoma (Kacker; Taskin, 1996). Infiltrating lipoma should also be differentiated from myofibroma, which exhibits a mixture of adipose and vascular spindle cells scattered among normal and mature adipocytes. The latter are scattered among the adipose tissue, but also form large sheets. Mitoses are not seen and there is no evidence of malignancy; however, ectatic blood vessels are a prominent component (Barker; Sudderick, 2008).
In the present case, the diagnosis was based only on the histopathological findings. However, complementary diagnostic exams, such as magnetic resonance imaging (MRI) and computed tomography (CT), assist in the precise delineation of the tumor and facilitate the diagnosis of the benign nature of the lesion and its intramuscular location (Nishida et al 2007; Salvatore et al, 2003; Matsumoto et al, 1999). CT is better than MRI for differentiation, whereas MRI is better for delineating the extent of the tumor. Occasionally, lipoma-like liposarcoma may be histologically confused with benign lesions. In such cases, imaging findings are helpful and often provide almost pathognomonic evidence of lipoma-like liposarcoma. Intramuscular lipoma, which is usually a spherical mass located in muscle, contains streaks of variable thickness with an occasional interruption on CT and magnetic resonance images. Lipoma-like liposarcoma, which is usually a spherical mass spreading over the intramuscular and intermuscular layers, contains fair hazy amorphous areas and soft tissue density septa on a CT image (Nishida et al 2007).
The ability of an intramuscular lipoma to infiltrate the adjacent muscle tissue and its rate of recurrence contribute further to a false clinical diagnosis of a malignant tumor, such as liposarcoma (Keskin et al, 2002). The fact that the mass of an intramuscular lipoma is uninodular, which can be seen using MRI, is also useful for differentiating intramuscular lipoma from liposarcoma (Matsumoto et al, 1999).
In the present case, surgical excision was performed with a margin of safety and there has been no recurrence of the tumor to date. The high rate of recurrence of intramuscular lipoma is due to its infiltrating growth. Meticulous surgical excision is the key to avoiding recurrence of the tumor (Akbulut et al, 2005; Thomas et al, 2002). According to Epivatianos et al (2000), although extra-oral intramuscular lipoma has a high rate of recurrence following surgical excision, oral intramuscular lipoma, despite being poorly delimited, rarely reoccurs when excised completely. However, close follow up of the patient is indicated. Akbulut et al (2005) report an absence of recurrence in a five-year period. Fregnani et al (2003) report no recurrences among 36 cases after a mean period of 26.5 months. After analyzing 40 cases of extra-oral intramuscular lipoma, Nishida et al (2007) report three recurrences four, six, and 11 years following surgery.
CONCLUSIONS
Dentists should be aware of the clinical characteristics and progression in order to differentiate malignant and benign tumors as well as to plan the correct treatment of oral lesions. Although rare, intramuscular lipoma may occur in the oral cavity, preferentially located on the tongue. Patient follow up is important due to the chance (albeit minimal) of recurrence of the tumor.
REFERENCES
1 Akbulut, M, Aksoy, A, Bir, F. (2005) Intramuscular lipoma of the tongue: A case report and review of the literature. Aegean Pathology Journal. 2, 146-9.
2 Barker, L, Lo, S, Sudderick, R. (2007) Gorlin´s syndrome presenting with myolipoma of tongue base. The Journal of Laryngology & Otology. 122, 1130-2.
3 Colella, G, Biondi, P, Caltabiano, R, Vecchio, G M, Amico, P, Magro, G. (2009) Giant intramuscular lipoma of the tongue: a case report and literature review. Cases Journal. 2:7906.
4 Colella, G.; Lanza, A.; Rossiello, L.; Rossiello, R. (2004) Infiltrating lipoma of the tongue. Oral Oncology Extra. 40, 33-5.
5 Epivatianos, A, Markopoulos, A K, Papanayotou, P. (2000) Benign tumors of adipose tissue of the oral cavity: A clinicopathologic study of 13 Cases. Journal of Oral Maxillofac Surgery. 58,1113-7.
6 Fregnani, E R, Pires, F R, Falzoni, R, Lopes, L A, Vargas, P A. (2003) Lipomas of the oral cavity: clinical findings, histologicalclassification and proliferative activity of 46 cases Journal of Oral and Maxillofacial Surgery. vol. 32, 49-53.
7 Freitas, M A, Freitas, V S, Lima, A A, Pereira Jr, F B. (2009) Intraoral lipomas: A study of 26 cases in a Brazilian population. Quintessence International. 40, 79-85.
8 Furlong, M A, Fanburg-Smith, J C, Childers, E L B. (2004) Lipoma of the oral and maxillofacial region: site and subclassification of 125 cases Maxillofacial Pathology. 98,441-50.
9 Kacker, A, Taskin, M. (1996) Atypical intramuscular lipoma of the tongue. The Journal of Laryngology & Otology.110, 189-91.
10 Keskin, G, Ustundag, E, Ercin, C. (2002) Multiple infiltrating lipomas of the tongue. The Journal of Laryngology & Otology.116, 395-7.
11 Matsumoto, K, Hukuda, S, Ishizawa, M, Chano, T, Okabe, H. (1999) MRI findings in intramuscular lipomas. Skeletal Radiology. 28, 145-152.
12 Moore, P L, Goede, A, Phillips, D E, Carr, R. (2001) Atypical lipoma of the tongue The Journal of Laryngology & Otology. 115, 859-86.
13 Nishida, J, Morita, T, Ogose, A, Okada, K, Kakizaki, H, Tajino, T, Hatori, M, Orui, H, Ehara, S, Satoh, A. (2007) Imaging characteristics of deep-seated lipomatous tumors: intramuscular lipoma, intermuscular lipoma, and lipoma-like liposarcoma. Journal of Orthopedics Science.12, 533-41.
14 Salvatore, C, Barberi, A, Vecchio, W D, Lanza, A, Tartaro, G P, Colella, G. (2003) Giant infiltrating lipoma of the face: CT and MR imaging findings. Journal of Neuroradiology. 24, 283-6.
15 Scolozzi, P, Lombardi, T, Maire, G, Pedeuteur, F, Richter, M. (2003) Infiltrating intramuscular lipoma of the temporal muscle. A case report with molecular cytogenetic analysis. Oral Oncology. 39, 316-22.
16 Tateyama, A K, Rossi, J M, Martins, M A T, Bussadori, S K, Fernandes, K P S, Lemos, J B D, Martins, M D. (2005) Lipoma bucal: relato de dois casos. Conscientiae Saúde. 4, 115-21.
17 Thomas, S, Varghese, B T, Sebastian, P, Koshy, C M, Mathews, A, Abraham, E K. (2002) Intramuscular lipomatosis of tongue. Postgraduation Medicine Journal. 78, 295-7.
Copyright Priory Lodge Education Limitd 2010 -
First Published September 2010
Click
on these links to visit our Journals:
Psychiatry
On-Line
Dentistry On-Line | Vet
On-Line | Chest Medicine
On-Line
GP
On-Line | Pharmacy
On-Line | Anaesthesia
On-Line | Medicine
On-Line
Family Medical
Practice On-Line
Home • Journals • Search • Rules for Authors • Submit a Paper • Sponsor us
All pages in this site copyright ©Priory Lodge Education Ltd 1994-


