Medical Ethics
Dr Ben Green
Four Bioethical Principles
The four bioethical principles have been described as:
- Autonomy - respect for the individual and their ability to make decisions with regard to their own health and future. Actions that enhance autonomy are thought of as desirable and actions that 'dwarf' an individual and their autonomy are undesirable.
- Beneficence - actions intended to benefit the patient or others
- Non-maleficence - actions intended not to harm or bring harm to the patient and others
- Justice being fair or just to the wider community in terms of the consequences of an action
Summary Points
Four bioethical principles that are often used in medical ethics analyses are autonomy, beneficence, non-maleficence and justice.
- Where these principles are invoked they must be correctly used and defined.
- Other methods of analysis can produce a more holistic and three-dimensional approach to problems
Confidentiality
Confidentiality is not a single ethical principle in itself, rather it is linked in to several bioethical principles.
Confidentiality shows a respect for an individual's autonomy and their right to control the information relating to their own health. In keeping information about the patient secret the doctor is acting beneficently. Disclosing information without the patient's consent can damage the patient. For instance if a doctor were to reveal privileged information about a celebrity patient to the newspapers then this would be the very reverse of beneficent i.e. malificent Maintaining confidentiality can therefore also be seen as non-maleficent.
Breaking confidentiality
Confidentiality may be broken in certain circumstances. For instance if there is a risk to a third party this may overrule the necessity to maintain confidentiality. Examples of this conflict of duty may be seen in psychiatry. A patient may, for instance, disclose to his doctor that he believes his sister is an evil witch. His delusion is also linked to a plan to kill her. The doctor must weigh up his duty to his patient to maintain confidentiality against a duty to protect the unknown sister. This dilemma involves a conflict between the principles of autonomy and non-maleficence outlined above.
The breaking of the confidence in the example above would be seen as reasonable at the time of writing in the UK and in the USA. However you could envisage a change in the prevailing ethos of the day, where the concept of confidentiality became more or less important or more or less restrictive. The details of the doctor-patient consultation might be seen as absolutely sacrosanct and so no details could ever be revealed to another individual. Conversely the consultation might be seen as transparent, and details might be shared without let or hindrance between healthy professionals and state officials.
In some cases the doctor may, at their own discretion, decide to disclose information. Examples could include:
- where serious harm may occur to a third party, whether or not a criminal offence, e.g. threat of serious harm to a named person
- where a doctor believes a patient to be the victim of abuse and the patient is unable to give or withhold consent to disclose
- where, without disclosure a doctor would not be acting in the overall best interests of a child or young person who is his/her patient and incapable of consenting to disclosure
- when, without disclosure the task of preventing or detecting a serious crime by the police would be prejudiced or delayed
- when, without disclosure the task of prosecuting a serious crime would be prejudiced or delayed (e.g. a patient tells you that he killed someone several years ago)
- where a doctor has a patient who is a health professional and has concerns over that person’s fitness to practice and posing a serious
danger to patients in his or her care - where a doctor has concerns over a patient’s fitness to drive.
(Good Psychiatric Practice: Confidentiality [2000] Royal College of Psychiatrists)
Ethics should never be viewed as being interchangeable with the law. The law can be informed by ethics, and often is. Sometimes the law may fly in the face of established ethical principles, such as a law requiring a doctor to send incurable patients to a gas chamber. Such laws have existed in the past in Nazi Germany in the twentieth century, and doctors have complied with them. Other doctors have rebelled against such laws on ethical grounds. The law should never be a substitute for ethical reasoning.
In the UK the court can require a doctor to break confidentiality. This is, by and large, seen as reasonable by the courts, the public and the medical profession, and in this case the law conforms to the prevailing ethos or vice versa.
After a succession of cases in the UK and elsewhere where mentally ill people have murdered others there has been a shift away from the liberal principles of community care towards a much more structured legalistic framework of mental health law. The individual's right to confidentiality, sometimes a key issue in whether patients will approach psychiatrists for help, has been eroded. 'Good practice' espoused by the Government through its new and proposed legislation involves information about the patient being 'shared' by a whole network of professionals, Government agencies and 'carers'.
Statute laws in England and Wales which 'compel' doctors to disclose confidential information include:
(a) The notification of births and deaths under the National Health Service Act 1977 Section 124 and regulation (1982 SI. No. 286).(b) Notification of communicable disease covered by the Public Health (Control of Disease) Act 1984 and Public Health (Infectious Diseases) Regulations 1988.
(c) Notification of abortion — Abortion Regulations 1991, regulations 4—5 (duty of medical practitioner to notify of abortions carried out and circumstances in which further disclosure of that information may be required or requested).
(d) Serious accidents covered under the Health and Safety at Work etc. Act 1974. Regulations on the Reporting of Injuries Diseases and Dangerous Occurrence (1985 and 1989) and Road Traffic Acts.
(e) Acts of Treason and Intention to cause explosion to Her Majesty’s Dockyards.
(f) There are certain obligations to pass on information under the Mental Health Act 1983; Mental Health Patients in the Community Act 1995;
Mental Health Act (Scotland) 1984; Mental Health NI Order 1986; and the Mental Treatments Acts (Ireland) 1945—61.
(g) Section 1 — AIDS Control Act 1987 (duty of health authority and others to make reports of number, but not the identity of, persons with AIDS or known to be HIV antibody positive).
(h) Section 18 — Prevention of Terrorism Act 1989 (power to require the production of information from any person, making it an offence to fail to volunteer that information).
(i) Road Traffic Act 1988 (S.172), which may require an attending doctor to provide the identity of patients he/she has treated following a road traffic
accident.
Summary Points
- Confidentiality involves a respect for autonomy and also beneficence towards the patient and a desire to act non-maleficently
- Confidentiality is not an ethical principle in itself. It can be characterized as a duty by some health professionals.
- The concept of confidentiality is elastic and may be interpreted rigidly or less strictly with information 'sharing' by a team
- Most countries have laws to enable the breaking of confidentiality
- Breaking confidentiality to protect the safety of a third party is seen as reasonable
- The law is not necessarily interchangeable with a system of ethics
- The ethos of a group can change over time
Relationships with Patients
Most ethical codes forbid doctors and nurses to have sexual relationships with patients. Professional bodies view these relationships as 'serious misconduct' and erstwhile professionals may be expelled from professional bodies and thus stopped from practicing their profession. The untoward consequences of sexual relationships therefore deter most practitioners from 'unprofessional' conduct.
Why are such relationships frowned upon? The professionals is in a privileged position and there is a profound power differential between the patient and the doctor. Although current 'politically correct' thinking dictates that the doctor and patient are 'partners' in diagnosis and treatment, in reality the patient is very dependent and vulnerable. Although it would be politically incorrect of me to say so, in this aspect the professional is responsible for the conduct of the relationship, in something almost of a parental role.
A sexual relationship based on this power differential could be viewed as abusive, in which there is ill-informed consent leading to a lack of autonomy. The doctor would not be respecting the patient's autonomy is proceeding with the relationship, however they chose to frame their behaviour.
In avoiding such relationships the professional is acting non-maleficently.
Summary Points
- Maintaining the professional relationship shows a respect for autonomy, beneficence towards the patient and a desire to act non-maleficently
- Sexual relationships with patients cannot be justified, are abusive and inherently harmful for the patient involved.
Ethics Tools: The Rings of Uncertainty
Medicine abounds with uncertainty. When does intrinsic asthma become extrinsic asthma? If diabetes is diagnosed at a blood glucose over 8mmol/l, where does this leave a patient with a glucose level of 7.98mmol/l? If a patient has a high Prostate Specific Antigen level how likely is he to have cancer? If a boy is unruly at 15 he may attract a diagnosis of conduct disorder, but if he is 16 he might be diagnosed instead as a personality disorder...so why does the diagnosis change when all that has changed is the patient's age?
At a personal level how certain are we that we ourselves know a set of facts (e.g. after revising for an exam) or how certain are we that we can perform a standard procedure. For instance a house officer might be very assured that they can take blood, but that would be very uncertain about whether they could perform a lumbar puncture without supervision. A Specialist Register in surgery might feel competent to perform an appendicectomy as an emergency procedure, but would feel extremely uncertain about performing a cardiac bypass operation alone.
The rings of uncertainty is a model which can be used to analyse this uncertainty and suggest ethical action. The model is described at length in David Seedhouse's book.
The Figure below shows how you could grade certainty, where A= No uncertainty or very high probability, B=some uncertainty, C= much uncertainty and D = total uncertainty.

How can this be used?
You could express the rings in the arena of competence as outlined above. Only where the certainty of competence is high could the doctor, then an expert, act in confidence in the best interests of the patient. In such a model of competence, the central area, A would be equivalent to Specialist Competence or Expert Competence. B might equal Shared competency, where actions might be best undertaken by say, a team of doctors, e.g. a medical firm with a house officer, SHO and SpR - they all have the mutual competencies of doctors, for instance you could expect they would all be able to pronounce a patient dead. C would indicate a level of competency where actions were best undertaken in teams - for instance with regard to deciding if child abuse has occurred - the team might be best at judging the issue rather than say a paediatrician working alone without the additional competency/skills of a social worker. In area D there may be no special competence or relevant skill. Such an individual might have no more or less skill than any adult member of the public.
How does this fit into ethics?
If we assume a duty of care exists with regard to a patient. A health care worker could be said to be acting ethically if they undertook some specialist skill on behalf of that patient if they were acting alone in area A or in a team with certainties of competence in areas B and C. They would be acting unethically perhaps if they undertook the procedure, but only had competencies in level D.
So, if I, Dr Green under took to perform an appendicectomy, I would be acting unethically. My level of competence is probably around level B or maybe C since I was once a house surgeon. This, of course assumes, that there is a health service or a satisfactory availability of surgically trained doctors who can do the procedure better than I. If I was on a desert island with one other person who had appendicitis, I would be the best person there to perform the appendicectomy and acting ethically. Context is important.
This leads us onto another way the rings can be used. Besides competencies, the rings can be expressed for resources.
A could equal adequate resources, B could equal Resources which require rationing, C could equal scarce resources and D no resources.
It might be ethical for a doctor to perform a kidney transplant if a suitable kidney (adequate resource) is found, but unethical to proceed with an inadequate resource (e.g. lamb's kidney from Sainsbury's). The arguments regarding scarce resources can get heated. Should money be spent on health promotion to reduce smoking and hence reduce heart disease or should it be spent on heart bypass operations for those who have smoked and developed cardiovascular disease as a result?
The rings could be expressed for Law. Perhaps Doctors should only act within areas of legally sound practice, but the law does not cover all eventualities, so what then?
Area A might equal legal practice where the law is gratifyingly precise (e.g. Statute law like the Mental Health Act) and there is no danger of criminal or civil action against the doctor. B could be an area where the law is reasonably predictable - where there are some legal precedents, that is to say case law that covers similar circumstances e.g. treatment for a patient who cannot consent but where a reasonably competent person would consent, say, for life saving treatment where the patient is unconscious. Area C might be an area where civil law is not predictable, say where Siamese twins need separating and one would die so that the other could survive, or the feeding against their will of an anorexic. In such circumstances the law can oscillate and uncertainty prevails. Area D is outside the law, where certain actions are clearly illegal e.g. murder.
The difficulty is that although ethical actions usually approximate to law and vice versa, this is NOT always true. For instance to take a glaring example, the Mental Health Law in Germany in the 1930s promoted the sterilisation and ultimately the killing of 'incurable' mentally ill people. The slogan involved was that they were 'life unworthy of life' and that the killing was a kindness. This reflected the ethos of the day and was legal. With our modern day perspective these killing actions by soldiers, doctors, professors and the public seem grossly unethical.
Exercise: Can you put together an ethical argument against these 'mercy killings'? Could you try and defend the German psychiatrists who acted in accordance with the legal health policy of the time? Does the fact that there was no particular treatment for mental illness excuse these acts? One treatment of the time was insulin coma. You can read about this historical treatment elsewhere in this site.
Finally perhaps the rings can be expressed for a kind of global ethical certainty where A is an uncontroversial and moral policy e.g. saving the life of a powerless stranger in an emergency, B might be a generally acceptable moral policy e.g. an NHS system offering emergency medical care to all without charge funded by general taxation, C might be a morally doubtful policy e.g. donating sperm for profit, D might be an immoral practice e.g. prescribing unnecessary (and explosive!) purgatives for a patient you don't like.
How can the rings be used to perform an ethical analysis?
The rings can be divided into quadrants, (or into as many areas as you choose to consider, becasue you could adapt them to say consider Communication or Knowledge as well). The diagram might then look like the one below. The individual anlaysis might consider each quadrant in turn for any particlar action fo intervention. Perhaps competence might be at an expert level, but resources are scarce, or a procedure might be frowned upon legally. The individual might only choose to act in cases where all certainties were in the central region i.e. where the procedure was ethically sound, legally acceptable, where resources were assured and where the individual's competence was at the expert level.

Exercise: Perhaps you could try and analyse whether you yourself would act in certain circumstances or the case of certain procedures using this tool. What if you were faced with a collapsed person in the street and asked to perform Cardiopulmonary Resuscitation? What if an SHO asked you to take some blood from an unconscious child?
Ethics Tools: The IFS Model
The IFS model is a visual tool to help analyse the consequences of an action on various levels and areas. The model is reproduced below:
An act is defined as an interaction between two individuals. The interaction may be so subtle that neither individual is aware of any action. This would for instance include unconscious interactions such as the transference and counter transference between patient and doctor. Conscious interactions might include a transaction such as a doctor examining and diagnosing a patient, a private broker buying healthcare from a specialist, or the referral of a patient between a GP and a consultant.
The interaction links both individuals and may have present and future ramifications for both.
Effects may ripple outwards from the interaction.
The diagnosis of a disease in an individual will probably have consequences for the family of friends, or the F subset of the Venn Diagram. Unless the two individuals are of the same family or group of friends there will probably be no overlap between these subsets. In small communities though this may not be the case. In a small island community, say, the doctor may well be part of the same group of friends or even family, in which case the above diagram would have to be amended.
The two individuals will usually be of the same society and so an overlap is presented here between sets. In a global community though it is possible that the interaction may be remote. For instance an important email consultation may occur between an international specialist and a distant patient. In this case the overlap in the above diagram would have to be amended.
Generally the individuals though will be of the same society and the same environment. The environment envelops individuals, families and their society.
An interaction may well seem at first analysis to involve only two individuals and extending this to the family and the society may seem initially pointless. However, even a circumscribed interaction may well ethically extend beyond the individuals. For instance a specialist may prescribe radiotherapy for a patient. The radiotherapy involves hazardous radioisotopes, which present risks to the radiotherapy technicians and to the staff who maintain radiotherapy machines (society) and those who must dispose of unused or unwanted radioactive waste in turn presenting certain risks to the environment. The prescription of antibiotics to an ill child with an upper respiratory tract infection may seem ethically to be an interaction purely between doctor and patient (and parent). However, an unwanted effect of the transaction may be a rise in the likelihood of the development of antibiotic resistant bacteria in the environment.
Let us see how the model works in a specific example.
Dr White is a doctor who must impart some bad news to a patient, Mr. Clitheroe. The patient is seen at the end of a clinic and given adequate time to discuss the diagnosis of bronchial cancer and the proposed treatment of chemotherapy. The appointment is an emotional one. Dr White leaves the clinic tired and emotionally drained. Mr. Clitheroe waits some time and then takes a taxi home and thinks over what he must tell his wife and children.
Dr White arrives home out of sorts and pours himself a drink. His wife notices that he is somewhat preoccupied and asks what the matter is. Dr White does not appreciate the sympathy and begins an argument about some irrelevant matter.
Mr. Clitheroe arrives home and after having a bath and a mug of tea tells his wife the unhappy news. Later on he tells his children and his best friend, John Marks. He begins to think about taking sick leave.
In this case we can see implications of the diagnostic transaction that only hours afterwards extend beyond the individuals (I). Both families are affected. Mrs. White has to bear the brunt of Dr White's ill humour after a fraught appointment(F). The Clitheroe family has to absorb the impact of the diagnosis(F). The implications ripple outwards as time progresses, washing over Mr. Clitheroe's friend Mr. Marks(F), and beginning to affect society as Mr. Clitheroe considers taking time off work (S).
Ethics Tools: The Ethical Grid
The Ethical Grid by David Seedhouse - you either love it or loathe it. But perhaps to love it or loathe it you first have to understand it before you can respond to it emotionally, and some people just find it difficult to get their heads round. The small diagram below is reproduced from Seedhouse's book and if clicked on will lead you to a larger and legible version. A forthcoming version of these notes will attempt to unravel its complexities.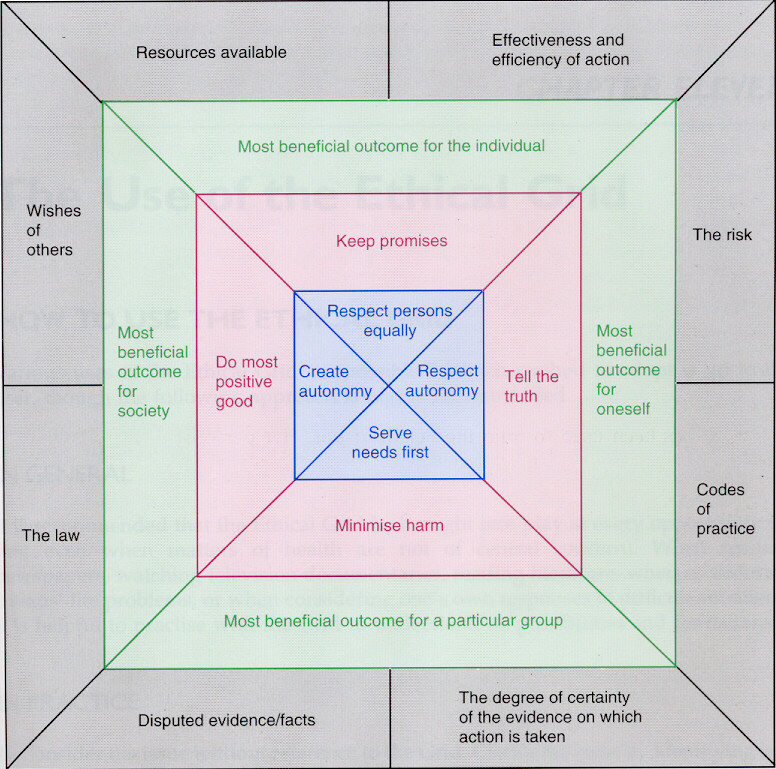
Duty
It has been argued that the only ethical acts are ones of 'duty'. Many answers referred to a duty to protect third parties, a duty to act in the patient's interests and a duty of confidentiality. The emphasis on duty is part of an area of ethics called deontology.
The question about Mr. Cousins and his seeking information about his wife was intended to cover the issue of confidentiality, but also two other duties - the duty to protect third parties and the duty to provide healthcare.
You will remember that Mrs. Cousins had a history of mental illness in her records and had assaulted her son and threatened Mr. Cousins with scissors.
A minority of answers did not pick up on these points and blithely told Mr. Cousins that he was not a patient and could not be helped. The response seemed almost like that of an automaton.
Most answers referred in some way to the risk that Mrs. Cousins might assault the son again and suggested that the father move away with the son or suggested a referral to police or social services. They at least had picked up the concept of a duty to protect others. There were several references to appropriate legislation such as the Children's Act.
Only a minority, (a disappointingly small minority), picked upon the fact that Mrs. Cousins could be relapsing and deserved treatment. Only one or two answers suggested that a psychiatrist might be involved or treatment of Mrs. Cousins attempted. There were one or two references to appropriate legislation such as the Mental Health Act.
The question about Mrs. Cousins was therefore only answered correctly by a small minority.
Summary points
· The emphasis on duty is part of an area of ethics called deontology.
· Doctors' duties are commonly held to include a duty to protect third parties, a duty to act in the patient's best interests and a duty of confidentiality
· Professional ethical duties are sometimes enshrined in legislation such as Mental Health Act and the Children's Act in the UK. No single Act of Parliament covers all of a doctor's duties.
· Professional statutory bodies such as the General Medical Council may list duties as they see them. There is something of an obligation for doctors to act ethically according to these codes of conduct.
Hippocratic Oath
The Hippocratic Oath was an oath supposedly originating with the ancient physician Hippocrates who founded a school of medicine in Kos. The oath was taken on graduation from medical school. The oath prescribed certain behaviours to protect the professional and their patients. Medical graduates no longer automatically swear the oath. Reference to modern ethical behaviours against the standards of this past code of conduct can be made, but only if the reference is clearly set in a historical setting or as part of descriptive ethics (where the ethos of past civilisations or the ethics pertaining to another country are considered).
The original version is:
I SWEAR by Apollo the physician and Aesculapius, and Health,
and All-heal, and all the gods and goddesses, that, according to my
ability and judgment, I will keep this Oath and this stipulation
-- to reckon him who taught me this Art equally dear to me as my
parents, to share my substance with him, and relieve his necessities
if required; to look upon his offspring in the same footing as my
own brothers, and to teach them this art, if they shall wish to learn
it, without fee or stipulation; and that by precept, lecture, and
every other mode of instruction, I will impart a knowledge of the Art
to my own sons, and those of my teachers, and to disciples bound by
a stipulation and oath according to the law of medicine, but to none
others. I will follow that system of regimen which, according to
my ability and judgment, I consider for the benefit of my patients,
and abstain from whatever is deleterious and mischievous. I will
give no deadly medicine to any one if asked, nor suggest any such
counsel; and in like manner I will not give to a woman a pessary to
produce abortion. With purity and with holiness I will pass my life
and practice my Art. I will not cut persons labouring under the stone,
but will leave this to be done by men who are practitioners of this
work. Into whatever houses I enter, I will go into them for the
benefit of the sick, and will abstain from every voluntary act of
mischief and corruption; and, further, from the seduction of females
or males, of freemen and slaves. Whatever, in connection with my
professional service, or not in connection with it, I see or hear,
in the life of men, which ought not to be spoken of abroad, I will
not divulge, as reckoning that all such should be kept secret. While
I continue to keep this Oath unviolated, may it be granted to me
to enjoy life and the practice of the art, respected by all men,
in all times. But should I trespass and violate this Oath, may the
reverse be my lot.
Some contemporary medical schools impose a revised version of the oath as an admonition and an affirmation to which their graduating classes assent. One version, approved by the American Medical Association, is as follows:
You do solemnly swear, each by whatever he or she holds most sacred
That you will be loyal to the Profession of Medicine and just and generous to its members
That you will lead your lives and practice your art in uprightness and honor
That into whatsoever house you shall enter, it shall be for the good of the sick to the utmost of your power, your holding yourselves far aloof from wrong, from corruption, from the tempting of others to vice
That you will exercise your art solely for the cure of your patients, and will give no drug, perform no operation, for a criminal purpose, even if solicited, far less suggest it
That whatsoever you shall see or hear of the lives of men or women which is not fitting to be spoken, you will keep inviolably secret
These things do you swear. Let each bow the head in sign of acquiescence
And now, if you will be true to this, your oath, may prosperity and good repute be ever yours; the opposite, if you shall prove yourselves forsworn.
The BMA updated the oath and produced this version in 1997:
The practice of medicine is a privilege which carries important responsibilities. All doctors should observe the core values of the profession which centre on the duty to help sick people and to avoid harm. I promise that my medical knowledge will be used to benefit people's health. They are my first concern. I will listen to them and provide the best care I can. I will be honest, respectful and compassionate towards patients. In emergencies, I will do my best to help anyone in medical need.
I will make every effort to ensure that the rights of all patients are respected, including vulnerable groups who lack means of making their needs known, be it through immaturity, mental incapacity, imprisonment or detention or other circumstance.
My professional judgment will be exercised as independently as possible and not be influenced by political pressures nor by factors such as the social standing of the patient. I will not put personal profit or advancement above my duty to patients.
I recognise the special value of human life but I also know that the prolongation of human life is not the only aim of healthcare. Where abortion is permitted, I agree that it should take place only within an ethical and legal framework. I will not provide treatments which are pointless or harmful or which an informed and competent patient refuses.
I will ensure patients receive the information and support they want to make decisions about disease prevention and improvement of their health. I will answer as truthfully as I can and respect patients' decisions unless that puts others at risk of harm. If I cannot agree with their requests, I will explain why.
If my patients have limited mental awareness, I will still encourage them to participate in decisions as much as they feel able and willing to do so.
I will do my best to maintain confidentiality about all patients. If there are overriding reasons which prevent my keeping a patient's confidentiality I will explain them.
I will recognise the limits of my knowledge and seek advice from colleagues when necessary. I will acknowledge my mistakes. I will do my best to keep myself and colleagues informed of new developments and ensure that poor standards or bad practices are exposed to those who can improve them.
I will show respect for all those with whom I work and be ready to share my knowledge by teaching others what I know.
I will use my training and professional standing to improve the community in which I work. I will treat patients equitably and support a fair and humane distribution of health resources. I will try to influence positively authorities whose policies harm public health. I will oppose policies which breach internationally accepted standards of human rights. I will strive to change laws which are contrary to patients' interests or to my professional ethics.
Summary points
- The Hippocratic Oath was traditionally an oath taken on graduation from medical school.
- Medical graduates no longer automatically swear the oath.
- Reference to the oath can be made in a historical sense as part of descriptive ethics.
- Updated versions exist, but are not universally in use
Books
Suggested books include:
***Ethics: the heart of health care by David Seedhouse. Second Edition. Rather uneven book, but has some useful analysis tools in, namely the Ethical Grid and Rings of Uncertainty / Competence. Buy it on-line
****Teach Yourself Ethics by Mel Thompson. Describes philosophy of ethics well, is concise and well written. Buy it on-line
****Law for Doctors by Margaret Branthwaite. Brief current overview of main case and statute law relating to a range of civil and criminal problems. Obviously not pure ethics, but indicative of English law related to some difficult issues. Buy it on-line
Version 2.0 Published July 2001
Home • Journals • Search • Rules for Authors • Submit a Paper • Sponsor us
All pages copyright ©Priory Lodge Education Ltd 1994-

