
Bianca Marques Santiago, DDS
Postgraduate student, Department of Pediatric Dentistry and Orthodontics, School
of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil.
Daniella Della Valle Sigmaringa, DDS, MSD
Master of Pediatric Dentistry, School of Dentistry, Federal University of Rio
de Janeiro, Rio de Janeiro, Brazil.
Lucianne Cople Maia, DDS, MSD, PhD
Associate professor, Department of Pediatric Dentistry and Orthodontics, School
of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil.
Corresponding author: Lucianne Cople Maia - Av. Marques do Paraná, 189/1804, Centro, Niterói, Rio de Janeiro, Brazil. Zip Code:24030-210. Telephone number: 55(21)2629-3738. E-mail address: rorefa@microlink.com.br
Abstract
The smile is very important for adults as well as for children and their guardians.
Its harmony could be negatively influenced by the presence of dental anomalies
like alterations in shape, size, position, color or texture. In this article
a case of a single unilateral peg-shaped maxillary lateral incisor is described
along with the conservative treatment proposed. The esthetic approach is reported
step by step and also discussed.
Introduction
A peg-shaped lateral incisor could be defined as a tooth with reduced mesio-distal
diameter and with proximal surfaces converging markedly in the incisal direction
(1). Generally, its diameter is reduced from the cervix to the incisal edge
(2). The inheritance of peg-shapped upper lateral incisors has been rather commonly
assumed to be associated with the genetic mechanism that causes the missing
of upper lateral incisors (1). Grahnen (3) claimed that this shape and size's
alteration is a modified manifestation of the genotype that causes hypodontia.
The available literature suggests that missing and peg-shaping of upper lateral
incisors are different expressions of one dominant autossomal gene (1,3).
The prevalence rate of peg-shaped permanent lateral incisors in the general
population ranges from slightly less than 1% to slightly more than 2 % (1,4).
No significant sexual differences in the frequencies have been found although
the frequencies in the women are, on an average, slightly higher (1). It can
be unilateral (1,5), mainly on the left side of the maxilla (6), or bilateral
(1,5). It has not been reported any kind of race predilection in the reviewed
literature.
Conical crown-size reduction of the maxillary lateral incisor is usually associated
with other dental anomalies like tooth agenesis (4,7), maxillary canine-first
premolar transposition (5), palataly displacement of one or both maxillary canine
teeth (8) and mandibular lateral incisor-canine transposition (9). In this cases
with concomitant dental anomalies, the prevalence suffers significant increase
from normal prevalence (1,5,8).
There are two treatment options for malformed lateral incisors: 1) to move the
maxillary canines forward and reshape them to simulate the extracted malformed
lateral incisors; 2) to stand the canines in a Class I relationship and to restore
the missing tooth structure by increasing the size of a peg-shaped lateral incisor
(10). The second option is more conservative and could be done by placing a
full-coverage crown on the lateral incisors (11) or reshaping them with acid
etch technique and bonded composite resin (10,12).
This paper reports a case of single unilateral peg-shaped maxillary lateral
incisor along with the conservative treatment proposed, that is described step
by step and also discussed.
Case Report
An 8-year-old caucasian female was referred to the pediatric dental clinic of
a public university in Rio de Janeiro, Brazil by one of the public dental services
of the same county. Her mother's main complaint was the presence of a reduced
anterior tooth that affected her child's smile. The patient also showed dissatisfaction
about this situation when asked about it, and a slight introspection was noticeable.
Her medical history was uneventful, except for the presence of respiratory allergy.
Intraoral clinical examination revealed that the patient was in early mixed
dentition. The upper arch presented spaces among incisors and a peg-shaped right
lateral incisor (Fig. 1A e 1B).
FIGURE 1 - A) Intra-oral aspect, frontal view, presenting spaces among incisors; B) lateral view, note the peg-shaped right maxillary lateral incisor; C) panoramic radiograph.

The lower arch presented
amalgam restorations on the primary first molars. All other erupted teeth were
caries-free. Both primary canines and permanent first molars presented Class
I relationship. There were no soft tissues alterations and oral hygiene was
adequate.
Panoramic radiographic examination (Fig. 1C) demonstrated a complete dentition,
with no other suspect of dental anomalies on permanent teeth. The mother was
asked about the presence of similar anomalies in other family members, but reported
no one in the family had teeth resembling these presented by the child.

Since there was an esthetic dissatisfaction, treatment plan for the patient
included a composite resin restoration of the peg-shaped right lateral incisor.
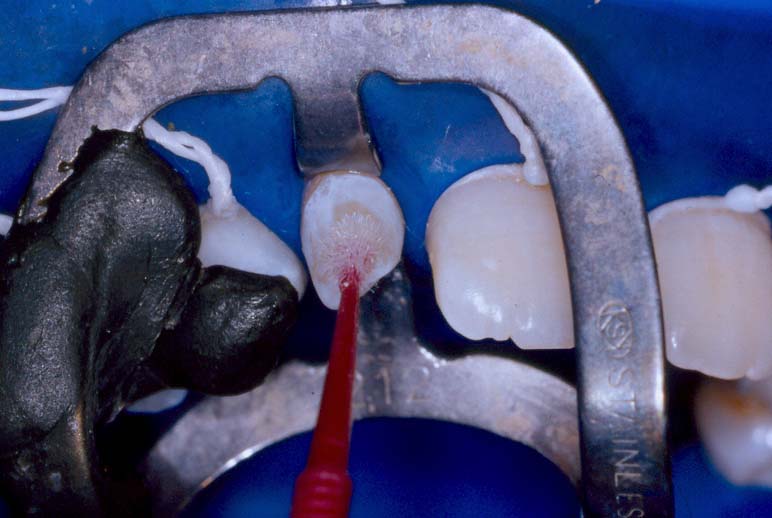
After tooth color selection, the patient was anesthetized and rubber dam was
placed to the teeth. A modified #212 clamp (KSK® - Dentech Corporation -
Tokyo - Japan) associated to molten graystick compound was used to stabilize
the rubber dam and also to gain access to the cervical region of the pegged
incisor (Fig. 2).
FIGURE 2 - Aspect of the rubber dam stabilized by a modified #212 clamp (KSK® - Dentech Corporation - Tokyo - Japan) associated to molten graystick compound.

No dental preparations were performed. After prophylaxis and protection of the adjacent teeth, acid etch (Conditioning Dental Gel® - 37%, Dentsply - Petrópolis - RJ/Brasil) was applied for 15 seconds (Fig. 3A).
FIGURE 3 - A) Acid etch conditioning for 15 seconds (Conditioning Dental Gel® - 37%, Dentsply - Petrópolis - RJ/Brasil); B) Placement of a primer- bonding agent (Prime & Bond® NT, Dentsply - Petrópolis - RJ/Brasil).

Then, the tooth was rinsed and dried and a primer-bonding agent (Prime & Bond® NT, Dentsply - Petrópolis - RJ/Brasil) was placed (Fig. 3B) and light cured for 20 seconds.
After that, the composite resin was applied through incremental layers (Fig. 4A).
FIGURE 4 - A) Placement of an increment of the opaque micro hybrid composite resin (Esthet X - A2O, Dentsply - Petrópolis - RJ/Brasil); B) Aspect after the placement of the last increment of a micro matrix composite resin (Estheth X - A2, Dentsply - Petrópolis - RJ/Brasil).

An opaque micro hybrid composite resin (Esthet X - A2O, Dentsply - Petrópolis - RJ/Brasil) was used to simulate the missing dentin and posteriorly, a micro matrix composite resin (Estheth X - A2, Dentsply - Petrópolis - RJ/Brasil) was applied superficially to simulate enamel (Fig. 4B). Each increment was light cured for 20 seconds.

Resin excesses were firstly removed with a surgical blade #12 (Fig. 5A) and
secondly with finishing diamond burs (KG Sorensen - São Paulo - SP/Brasil)
like 2200F diamond, that also helped on the sculpture (Fig. 5B).
FIGURE 5 - A) Finishing with a surgical blade #12; B) Final sculpture with finishing diamond burs (2200F - KG Sorensen - São Paulo - SP/Brasil).


Polishing was made with discs (Sof-lex®, KG Sorensen - São Paulo - SP/Brasil). After removing the rubber dam, occlusion and esthetics were checked and verified. Her guardian was advised to not allow the child to ingest any liquid or food containing corants for the first 24 hours after restoration.
The patient became very happy with the final result (Fig. 6A and 6B) and her
mother also commented on the natural look of the restoration. Patient's follow-up
visits are being scheduled twice a year.
FIGURE 6 - A) Final aspect of the composite resin restoration, frontal view; B) Lateral view of the peg-shaped right lateral incisor after composite resin restoration.


Discussion
Peg-shaped maxillary lateral incisors could be responsible for smile implications,
that varies from case to case, but could also cause alterations on psychological
behavior. A patient could be shy or even avoid social contacts depending on
the alteration degree (13,14). Children may demonstrate esthetic dissatisfaction
(16) as well as adults (15). Therefore, any esthetic problem that influences
social and personal relationships must be corrected, whenever possible (13,14,
15).
The case presented could be considered as an example of slight introspection
caused by a peg-shaped maxillary lateral incisor. The guardian reported that
her child was very vain and worried about her appearance, being anxious for
a solution to her conical crown-size reduced tooth. It is necessary to emphasize
that in this case the mother was even more anxious than the child, which is
usually common in pedodontic practice (16).
Literature has reported a higher prevalence of peg-shaped upper lateral incisor
in females (1,4), which corresponds to the case presented. Kook et al. (6) in
their study found it to occur more frequently on the left side of the maxilla,
however the current case presented a right pegged lateral. Many previous reports,
in the reviewed literature, have described the association between the presence
of peg-shaped maxillary lateral incisor and other developmental anomalies (1,4,5,7,8),
which increases its prevalence (1,5,8). So, the case reported is some kind of
unusual since panoramic radiographic did not reveal any missing teeth or other
dental anomaly.
Treatment plan consisted in retaining peg-shaped right maxillary lateral incisor
and reshaping it with bonded composite resin. This conservative option was chosen
because it preserves tooth structure once it is not necessary to make any preparations
on tooth, like the ones needed for the crowing technique (11). In addition,
this technique is not time consuming like orthodontic approach (10), which was
discarded since the patient was in the early mixed dentition still with the
presence of primary canines and the permanent first molars in Class I relationship.
Others advantages of this esthetic bonding procedure are the small cost when
compared to indirect technique and the fact that this kind of procedure is reversible
(17), allowing other treatment approaches in the future if necessary.
Nevertheless, bonding procedures like the one proposed need some cautions. The
rubber dam is an imperative step since it must not exist saliva or crevicular
fluid. It is necessary to check the occlusion (10) and to observe contralateral
tooth to simulate it and give a natural appearance to the tooth restored by
careful sculpture.
The authors of the present case agree with Miller et al. (10) that treatment
choice should be made on the basis of some considerations: need for extractions,
posterior relationships, position of the canines at the time of diagnosis; and
add others like patient's age, dentition's stage and patient's esthetic needs.
Conclusion
Direct composite resin restoration is a worthy conservative treatment option
to restore peg-shaped maxillary lateral incisors to normal contours. This esthetic
bonding procedure gives a natural look and improves smile, favoring esthetics
that is a current need nowadays and an important influence factor on personal
and social relationships.
References
1. Alvesalo L., Portin P. The inheritance pattern of missing, peg-shaped, and
strongly mesio-distally reduced upper lateral incisors. Dental Aktieselskabet
1969; 18(6): 563-75.
2. Le Bot P., Salmon D. Congenital defects of the upper lateral incisors (ULI):
consition and measurements of the other teeth, measurements of the superior
arch, head and face. Am J Anthrop 1977; 46:231-44.
3. Grahnen H. Hypodontia in the permanent dentition. Odont Revy 7:supp.3, 1956.
4. Meskin L.H., Gorlin R.J. Agenesis and peg-shaped permanent maxillary lateral
incisors. J Dent Res 1969; 27:563-73.
5. Peck L., Peck S., Attia Y. Maxillary canine-first premolar transposition,
associate dental anomalies and genetic basis. Angle Orthod 1993; 63(2): 99-109.
6. Kook Y.A., Park S., Sameshima G.T. Peg-shaped and small lateral incisors
not at higher risk for root resorption. Am J Orthod Dentofacial Orthop 2003;
123(3): 253-8.
7. Villani S., Stellzig A., Komposch G. Ipodontia: considerazioni sulla terapia
ortodontica nell'agenesia dell'incisivo laterale superiore permanente. Minerva
Stomatol 1995; 44(5): 211-22.
8. Peck S., Peck L., Kataja M. Prevalence of tooth agenesis and peg-shaped maxillary
lateral incisor associated with palatally displaced canine (PDC) anomaly. Am
J Orthop Dentofacial Orthop 1996; 110(4): 441-3.
9. Peck S., Peck L., Kataja M. Mandibular lateral incisor-canine transposition,
concomitant dental anomalies, and genetic control. Angle Orthod 1998; 68(5):
455-66.
10. Miller W.B., McLendon W.J., Hines F.B. Two treatment approaches for missing
or peg-shaped maxillary lateral incisors: A case study on identical twins. Am
J Orthod Dentofac Orthop 1987; 92(3):249-56.
11. Schmitz J.H., Coffano R., Bruschi A. Restorative and orthodontic treatment
of maxillary peg incisors: a clinical report. J Prosthet Dent 2001; 85(4):330-4.
12. Kazemi R., La Vecchia L.J. Restoration of peg-shaped lateral incisor with
acid etch technique. Georgetown Dent J 1979; 53(2): 43-4.
13. Baldwin W.C. Appearance and esthetics in oral health. Community Dent Oral
Epidemiol 1980; 8:244-56.
14. Jenny J., Proshek J.M. Visibility and prestige of occupations and the importance
of dental appearance. J Canadian Dent Assoc 1986; 12:987-989.
15. Neumann L.M. et al. Dental esthetic satisfaction in adults. J Am Dent Assoc
1989; 23:641-51.
16. Silva V.S., Barcelos R., Souza I.P. Perceptions of pediatric patients and
guardians about prosthetic appliances. J Clin Pediatr Dent 2002; 27(1): 87-90.
17. Miller T.E., Connely M.E. The diastema dilemma: an orthodontic approach
utilizing resin-bonded restorations. J Prosthet Dent 1996; 8(5): 206-14.
| Click on these buttons to visit our journals | ||||||||
| Psychiatry On-Line | Dentistry On-Line | Vet On-Line | Chest
Medicine On-Line | GP On-Line | Pharmacy On-Line | Anaesthesia On-Line | Medicine On-Line | Family
Medical Practice On-Line |
All pages copyright ©Priory Lodge Education Ltd 1994-2004.