Stimulus Dosing, Electrode Position and Stimulus Waveforms
The science in this area is generating a multitude of terms that are difficult to properly understand.
Glossary of Stimulus Related Terms
Glossary of Stimulus Related Terms
- Stimulus Dose
- To trigger a seizure an electric current is passed for a few seconds. The stronger the charge (strength being measured in volts or potential difference), the wider the pulses used (measured in milliseconds) and the longer this happens for (measured in seconds) adds up to the total energy applied. The total energy applied is measured in milliCoulombs.
- Threshold
- The lowest Stimulus Dose that leads to a bilaterally visible seizure longer than the minimum accepted duration (in our unit 15 seconds)
- Bilateral/Unilateral
- A bilateral seizure is one that is visible both sides of the body. The brain is in two halves, the right half controls the left side of the body and vise versa. A bilaterally visible seizure must therefore be a seizure that is happeneing on both the right and left side of the brain.
A bilateral stimulation is when the energy is applied across the head at the temporal areas. It is not thought to matter which direction the energy flows (sometimes it flows both ways alternately during one stimulation). A unilateral stimulation tends to be energy being applied only to the RIGHT side of the brain- but the resulting seizure still must be bilateral and of adequate duration
- Seizure Duration
- This part is odd. The measured seizure duration has not been shown to relate to how effective ECT is. However where EEGs have been looked at, longer clearer seizures are associated with better results than shorter ones. Most units have a lower cut off below which they deem a seizure to be insufficient. It was 25 seconds a few years ago in the UK, but we in Chester use 15seconds at present
- Impedance
- When electrical energy flows, some of it is lost as heat (and in the case of a lightbulb, light). The more 'resistance' an electrical circuit has, the more energy is lost. New ECT machines measure the 'resistance' (better termed impedance when using this type of waveform) and vary the machine settings according to how much impedance they find. Impedance measured before treatment is called the 'static impedance'. Once treatment starts the measured impedance falls dramatically (The dynamic impedance is usually afew hundred ohms). Before treatment a VERY high static impedance may mean the electrodes are broken, or contact is poor. A very LOW impedance indicates a short circuit. In either case the machines will not deliver their stimuli. By checking static impedance routinely you are checking the machine, the cables, and the electrical connection with the patient.
There is increasing recognition that the original belief, that a bilateral seizure was both necessary and sufficient to ensure that ECT would be effective (Cronholm BJ, Ottosson JO: Experimental studies of the therapeutic action of electroconvulsive therapy in endogenous depression. Acta Psychiatr Neurol Scand Supplement 145, 1960, pp 69-97.) is no longer true.
Work on using 'ultra-brief' pulses is beginning to suggest it might be possible to stimulate specific areas of brain and get response without a generalised seziure. Meanwhile however the standard way of stimulating is to find the actual seizure threshold and then treat the patient some way above this value.
The procedure of 'Stimulus Dosing', refers to the establishing, for each individual patient, a particular energy dose tailored to their own needs. For bilateral ECT (which means ECT given by stimulating from one temple to the other) this is considered to be the minimum energy needed to trigger a bilateral (visible on both side of the body) seizure of a more than minimum duration - multiplied by 1.5 (in other words, the use of 150% of the patients 'threshold').
Seizure threshold may vary from as low as 5mC to above 1200mC. However the TYPE of stimulus you use is important. Narrower pulses are better at evoking seizure activity then wider ones even given the same energy setting. Thus 'threshold' as a term is meaningless unless it includes both the electrode position AND the stimulus parameters.
Electrode Position
The objective of ECT is still to generate a seziure. The nature of epileptic brain activity is that it spreads across the surface of the brain (it generalises). Since it covers the entire brain, the assumption is that the point the seizure starts is not relevent.
Five different electrode positions are described consistently in the literature, of which three are in relatively regular use.
ECT Electrode Positions
- Bilateral (Bitemporal)
- One electrode is placed on each side of the head at a point (3) four centimeters perpenedicular to the middle of a line connecting the external ear canal with the angle of the eye.
Sobin C, Prudic J, Devanand D, Nobler M & Sackeim H (1996), "Who Responds to Electroconvulsive Therapy? A Comparison of Effective and Ineffective Forms of Treatment." (British Journal of Psychiatry 169,(3) ,322-8) reviewed two studies (with comprehensive exclusion criteria) looking at the effectiveness of unilateral v bilateral ECT. By looking at the patients that received the 'effective' forms of treatment categorised separately with 'retarded/non retarded', 'agitated/not agitated' or 'psychotic' /non psychotic depression relative outcomes associated predictive features were examined. Contrary to the accepted view, being in any of the three groups did not predict a good response. However the groups randomised to ineffective treatments did respond significantly less well (a tautology in this instance of course) suggesting that the study should have been powerful enough to show change that was present. [26 references]
- Unilateral d'Elia
- Right handed people are usually left brain dominant - hence unilateral stimulation of the right side can spare some side effects that relate to language (which is a left brain job). Half of all left handed people are also left dominant. Hence unilateral ECT uses the temporal position detailed with 'bilateral ECT on the right (3), with the second electrode one inch ipsilateral to the vertex of the scalp (1) The American Psychiatric Association Task Force on ECT (1990).
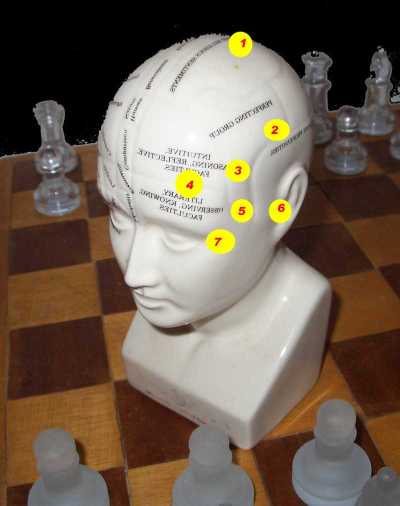
- Lancaster Unilateral (not used)
- The earliest form of unilateral used the left temporal position (3), as above, but the second electrode was three or so inches higher - over the parietal area (2). It is thought that most of the energy flowed through skin and meninges and didn't reach the brain.
Isaac Frost and West Cheshire Hospital

LANCASTER et al 1958 published the first controlled study of RUL using the temperopariental (or Lancaster) placement - Orientation and recall returned significantly faster after RUL ECT. But BILATERAL was 17% better (non sig). LANCASTER NP, STEINERT RR, FROST I: Unilateral electroconvulsive therapy. J Ment Sci. 104: 221-227, 1958
- Bifrontal
- Using two electrode, one above each eye (4), is considered by some to reduce the liklihood for cogntive side effects. The electrodes are howver still quite close together. This position is under review but has not been adopted widely. In Bailine SH, Rifkin A and Kayne E (2000) in "Comparison of Bifrontal and Bitemporal ECT for Major Depression", (The American Journal of Psychiatry, 157:121-123) report that higher energies are nmeeded to induce a seizure (x5) but treatment may be associated with fewer adverse conitive changes (and less risk to teeth). The authors observe that a number of machines however are not capable of sufficiently high output. Of 48 clients studied here 47 were in remission after 12 treatments. Mini Mental State scores were worse in the bitemporal group.
Max Fink wrote in the "Psychiatric Times" in 2005 about bifrontal ECT.
Two additional articles both retrospective support the (possibly reduced) efficacy and lower side effect profile of bifrontal. Little J et al (2004) "Bifrontal electroconvulsive therapy in the elderly". Journal of ECT 20:6, 139-141. and Bakewell C et al (2004), "Comparison of clinical efficacy and side effects for bitemporal and bifrontal electrode placement in electroconvulsive therapy". Journal of ECT 20:9, 145-153.
- LART
- The Left Anterior Right Temporal is a hybrid of Bitemporal and Bifrontal ((3) and (4) on opposite sides of the head). There is relatively little evidence for this position divised by Swartz as yet- but intuitively it does spare the left temporal (speech) area. For more information on the use of LART look at this document on the THYMATRON (ECT Machine) website called 'ECT Dosing by the Benchmark method' (Swartz, undated) also if you have a subscription to the Journal Of ECT click here (The Journal of ECT - Fulltext: Volume 19(2) June 2003 p 110-114) and here (The Journal of ECT - Fulltext: Volume 20(2) June 2004 p 127-129)
In every case the contact between the electrode and skin should be cleaned, preferably with a mildly abrasive, alcohol-free agent, and then made good with electrode paste or gel. Older electrodes had gauze pads on them that were soaked in an electrolyte solution. Apart from being messy, and could lead to electrolyte shorting out the electrodes.
In the USA electrodes tended to be held in place with a rubber head band - but latterly disposable stick on electrodes are used. In the UK separately held electrodes are preferred - although stick on electrodes are being introduced in some places.