1. Uday N. Reebye, DMD, MD .04, Former
Resident at Boston Medical Center, Department of Oral and Maxillofacial Surgery,
currently a medical student at University of North Carolina at Chapel Hill.
2. Michael J. Hunter, DMD, Assistant Professor of Oral and Maxillofacial Surgery
Boston Medical Center, Private practice, North Andover, MA.
3. David A. Cottrell, DMD, Director of Resident Training Program, Director of
Resident Research, Associate Professor of Oral and Maxillofacial, Boston Medical
Center
Please send all correspondence to:
Dr. Uday Reebye, 622 Edisto Ct,
Chapel Hill, NC 27514
Telephone: 919-932-4425
Both medicine and dentistry have generalists who serve as primary care providers and specialists to diagnose and treat complex cases. In medicine, 85% of physicians are specialists, which has resulted in a severe shortage of primary care providers. Historically, the abundance of medical specialists and relatively few primary care physicians have made it easy for individuals with traditional indemnity insurance to self refer to medical specialists even for minor problems. With the increased prevalence of Health Maintenance Organizations (HMO's), an emphasis has been placed on primary care treatment. In fact, many HMO's actively discourage specialist referrals by providing financial incentives to primary care providers to limit referrals to specialists. As dental managed care plans have become more common, the "gate keeper" medical model has been frequently adopted for dental plans.
Dentistry differs from medicine in that only 20% of dentists opt for specialty training, allowing adequate access to general dental care. Additionally, the very nature of dental care makes it more difficult to self-refer. For example, an individual with a toothache may have difficulty discerning whether a simple filling, root canal, periodontal treatment or an extraction is needed for appropriate treatment. This fact, coupled with the availability of general dentists, makes it uncommon for patients to self refer to most dental specialists. Still, dental managed care plans employ financial incentives developed for medical plans to limit referrals to specialists.1 According to the 1995 Managed Care Marketplace Information Survey, almost one third of private dental practitioners participated in at least one managed care plan. Although the future of dental managed care is uncertain, if the penetration of dental managed care plans increases as many predict, the potential impact of these restrictions will assume increasing importance to dentists, policy makers and the public.
Patients requiring oral care generally seek help and advice from their general practitioners. The decision to refer to a specialist is usually made by the general practioner.2,3 This trend will continue with the increased penetrance of managed care. Few studies have assessed the factors that influence dentists' decisions to refer surgical cases, and their self-reported competency in performing these procedures. The purpose of this study is to determine the self-perceived threshold for referral to a specialist for oral surgical needs.
This study consisted of Boston area
dentists. Six hundred dentists were selected at random to receive a cover letter
stating the objectives of the study and a questionnaire containing sixteen clinical
cases. Data collection stopped at 200 hundred respondents. Improperly filled
questionnaires and practitioners indicating post-graduate training were discarded
from the study. One Hundred and twenty eight respondents qualified for data
collection and comparison. The average age of respondents was 38 years with
the minimum age being 29 years and the maximum age being 59 years. The average
year of graduation was 1985, ranging from 1962 to 1996. The average years in
practice of the sample were 10.6 years with a range of 1 to 34 years. Among
the respondents, 96 (75%) were male and 32 (25%) were females. When the sample
was divided into 2 age groups, 86 (68.8%) fell into the age group 25-40 years
old and 39 (31.2%) fell into the age group 41-60 years of age. The sample was
divided into two groups according to the number of years in practice. One hundred
and seven (84.9%) of practitioners had between zero - 10 years of clinical practice
and 19 (15.1%) had practiced for more than 11 years. Practitioners were asked
to respond to each case as they would in their current clinical practice. The
randomly arranged cases consisted of radiograph and a brief case history. Each
case differed in complexity and was grouped according to surgical difficulty
as follows:
Group I - simple dentoalveolar surgery
Group II - complex dentoalveolar surgery (includes any third molar)
Group III - cases requiring placement of an implant
Group I/IV - simple surgery in a medically compromised patient
Group II/IV -complex surgery in a medically compromised patient
Analysis:
SAS chi-square analysis and Fisher's Exact Test were used to verify or reject the null hypothesis that the groups in question were identical in their treatment modalities. The null hypothesis was tested against gender, age group, and years of practice at 95% ((=0.05) and 90% ((=0.10) certainty.
Results:
Treatment modalities, referral patterns and reasons for referral by general dentists to the five case categories (groups I, II, III, I/IV and II/IV) were compared. Data of these groups compared in this paper are statistically significant to the 95% ((=0.05) or 90% ((=0.10) certainty. Respondents were further subdivided according to gender, age, and years of clinical practice to evaluate if there were statistically significant differences between these groups.
The referral patterns of general dentists between the five categories were found to be statistically significant. Clinicians treated 75.5% of simple dentoalveolar surgery cases (group I), referring 16.6% to Oral Surgeons, 0.3% to Periodontists and 7.3% to "other". (fig.1). In dealing with complex dentoalveolar surgical procedures (group II), clinicians were far less aggressive. Only 41.7% of general dentists would treat these cases, and almost exclusively referred these cases to Oral Surgeons (57.1%) (fig.2).
Both simple and complex dentoalveolar surgeries in medically compromised patients (group I/IV, Group II/IV) showed marked increases in referrals to specialists compared to cases in which the patient had a non-contributory medical history. Fewer dentist, (38.8%) would treat simple dentoalveolar in medically compromised patients; referring them to Oral Surgeons (39.1%) and Periodontists (11.7%). Clinicians were conservative in their management of cases involving complex dentoalveolar surgeries in medically compromised patients. Only 22.6% of general practitioners would treat such cases themselves, with the remaining referred to Oral Surgeons (75.4%). (fig.3)
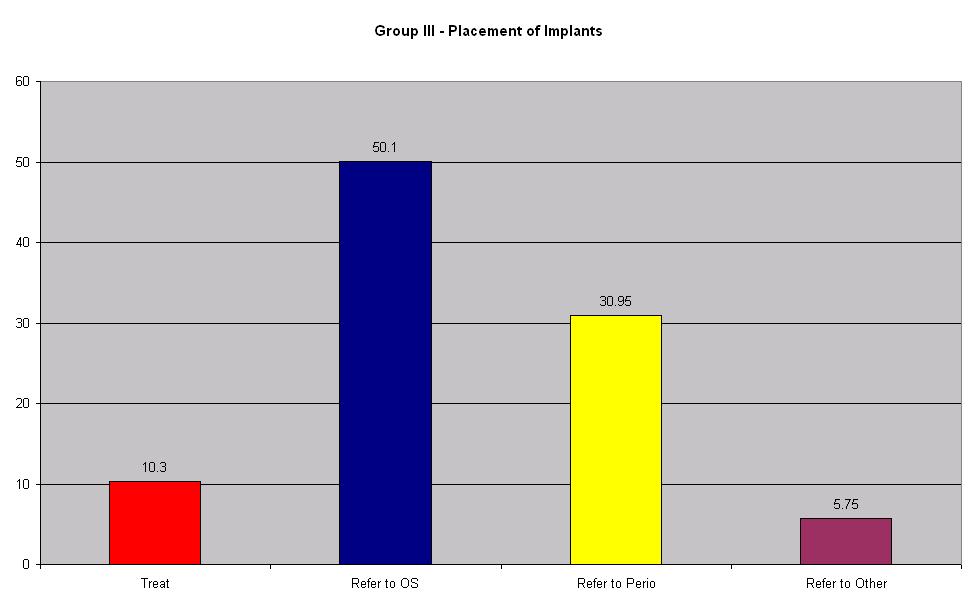
Cases requiring implants (group III) showed high referral rates. Only 10.3% of dentists would place implants themselves referring to oral surgeons (50.1%), and Periodontists (31.0%) (fig.4). Males would place implants more often (11.7%, (=0.05) than females (6.4%, (=0.05). Dentists cited inadequate surgical experience (58.7%), and a lack of proper surgical equipment (16.3%) as the main reasons for referring implant patients to specialists.
Gender differences existed in the treatment choices for oral surgical procedures on analysis of all groups (Groups I, II, III, I/IV, II/IV). Females referred more often than males treating 29.9% of cases requiring surgical procedures in contrast to males who treated 49.9%. (Fig. 5) Statistically significant differences ((=0.05) in referral patterns between males and females were seen in cases requiring; simple dentoalveolar surgery, (group I) and patients requiring the placement of implants (group III). Males tended to refer these cases less frequently. No gender difference was seen in patients requiring complex dentoalveolar surgery (group II). Although the date suggests that women are less aggressive in the treatment of oral surgical cases, the different of treatment modalities may be due to answers that are more honest by female clinicians then their male counterparts.
Clinicians' age was also a factor in determining the treatment modality of clinical cases. Respondents were divided into two groups "Young" and "Old" dentists. "Young dentists" being comprised of clinicians < 40yrs and "Old dentists" clinicians who are 40 years of age or older. Young dentist treated 77.0% of simple dentoalveolar surgeries (group I) compared to older dentists who treated only 70.5% ((=0.05) of these cases. Young dentist treated 28.5% of complex surgeries (group II) in contrast with 24.9% ((=0.01) of older dentists. According to the data, older dentists are more conservative then their younger counter parts. We can speculate that this difference may be due to the fact that older dentists are clinically more experienced and are aware or have experienced risks and complications of surgical procedures.
Common reasons for referral in simple and complex dentoalveolar surgery (groups I and II) were inadequate surgical experience (46.7, 33.5%), easy access to a specialist (29.9, 23.1%) and too time consuming (11.2, 19.6%). The main reasons in-group III was: inadequate surgical experience (58.7%), inadequate surgical equipment (16.3%), and easy access to a specialist (11.1%). In-group I/IV (medically compromised) the major reasons for referrals were: limited skill in the management of a medically compromised patient (28.9%), easy access to a specialist (25.2%), and inadequate surgical experience (16.7%). The main reasons for referral in-group II/IV (medically compromised) were; inadequate surgical experience (29.4%), easy access to a specialist (25.1%), and limited skill in the management of a medically compromised patient (13.1%).
This survey study describes factors that influence general dentists' decision to refer patients requiring dental alveolar surgery. In this sample, the major reason cited for referral was inadequate surgical experience. Also emerging as a powerful influence in the decision to refer was the availability of and ease of referral to specialist clinicians. Age and gender were also significantly associated with the decision to refer. Female dentists were more likely than their male counterparts to refer simple dentoalveolar surgeries and implant cases. Clinician gender differences disappeared as the complexity of the surgery increased with both genders reporting similar patterns of referral. Fewer clinicians felt prepared to perform surgeries on medically compromised patients regardless of the complexity. Oral surgeons continued to be the main referral source for both surgeries and implant cases.
The emerging influence of managed care in dentistry has the potential to impact access to specialists and consequently dentists' referral patterns. Currently, there are diverse models dictating the referral process in managed care systems. However, a universal theme is that the general dentist serves as the gatekeeper and often the general dentist assumes the financial risk for specialist referrals.4 In one model, there are financial penalties for over utilization of specialists. Another model rewards the primary care dentist for performing specialty care by providing payments in addition to their monthly capitation rate. Since these fees are less than specialists' fees, the managed care plan saves money. Both these models serve to limit access to care for specialty services beyond their level of expertise. Since, in this study, the vast majority of dental providers did not have adequate experience to perform complex extractions and only two thirds of the respondents reported adequate expertise to perform simple extractions, it is clear that these models would not ensure adequate oral health care for the public. Therefore, it is imperative that the existing competency level of general practitioners are considered when designing public policy for exodontia, dental alveolar surgery and management of the medically compromised patient.
Review of the data obtained from
our survey revealed five important points.
1. Most general dentists refer complex dentoalveolar surgery. This trend was
also seen amongst older and more experienced dentists. During clinical practice
most dentists have undertaken with difficult extractions, and have had to deal
with their complications.
These experiences are reflected in the higher referral for surgical extractions
to specialists.
2. There exists a gender difference in the referral patterns of female dentists
compared to their male counter parts in similar age groups and years of clinical
practice. This difference may be due to the willingness of the female dentist
to more honestly answer questions, than male dentists, rather than a difference
in training or skill level.
3. Most dentists refer implants to the Oral Surgeon or Periodontist.
4. Referrals for simple and complex surgical procedures were most often made
because of inadequate surgical experience. Easy access to an Oral Surgeon also
appears to be an important factor.
5. When designing dental health policy with regard to exodontia, dentoalveolar
surgery and management of the medically compromised patient, insurance companies
and public health administrators should consider the existing competencies of
the general practitioner. The results of this survey indicate general dentist
do not feel comfortable in treating patients requiring complex dentoalveolar
surgery (includes simple third molar extractions), or managing medically compromised
patients with oral surgery needs.
1. Cooke L, Davenport ES, Anderson
P: Changes in the referral pattern of child patietns from the GDS to the CDS
following the introduction of capitation in October 1990.General Dental Services.
Community Dental Services.Br. Dent. J. 185(11-12): 586-90, 1998 Dec 12-26
2. Worrall SF, Riden K, Haskell R, Corrigan AM: UK National Third Molar project:
the initial report. Br. J. Oral Maxillofac Surg. 36(1):14-8, 1998 Feb
3. Linden GJ: Variation in periodontal referral by general practitioners. J
Clin Periodontol. 25(8):655-61, 1998 Aug
4. Societies, Technology, Dental: The American Dental Trade Association looks
at dental reimbursement; responsible consumption of appropriate dental services.
Managed Care Task Force of the American Dental Trade Association. J Am Coll
Dent, 65(1):7-16, 1998 Spring.
Boston University School of Dental
Medicine,
Department of Oral and Maxillofacial Surgery
1. Uday N. Reebye, DMD, MD .04, Former
Resident at Boston Medical Center, Department of Oral and Maxillofacial Surgery,
currently a medical student at University of North Carolina at Chapel Hill.
2. Michael J. Hunter, DMD, Assistant Professor of Oral and Maxillofacial Surgery
Boston Medical Center, Private practice, North Andover, MA.
3. David A. Cottrell, DMD, Director of Resident Training Program, Director of
Resident Research, Associate Professor of Oral and Maxillofacial, Boston Medical
Center
Please send all correspondence to:
Dr. Uday Reebye, 622 Edisto Ct,
Chapel Hill, NC 27514
Telephone: 919-932-4425
Email: Uday_Reebye@med.unc.edu