Browse through our Journals...
Dentigerous Cyst: a review of 37 Cases
Dr. Ali H. Murad B.D.S.,M.Sc.
Assistant Prof. Head of Oral Pathology, College of Dentistry, University of Thamar
Abstract
A retrospective study looked at the features of dentigerous cyst clinically, radiographically and histopathologically in thirty-seven Iraqi patients from the archives of the Oral Pathology Department, College of Dentistry, University of Baghdad, for the period 1990-2000. The results showed that the mean age was (22.2)years, males were affected more than females in a ratio of 1.5:1. The maxillary canine area was the most specific site involved, followed by mandibular third molar. The most common clinical features were alveolar bone swelling, while pain is not a prominent feature. Radiographic appearance revealed a radiolucency associated with an unerupted tooth, in one case the cyst was associated with a supernumerary tooth in upper incisor area. Histologically, the cyst shows ameloblastic variation in only two cases.
Introduction
Odontogenic epithelium within the jaws act as the wellspring for a multiplicity of odontogenic cysts of varied clinical feature, histogenisis and biological behavior. Some of these lesions are relatively innocuous whereas others which originate by the separation of the follicle from around the crown of unerupted tooth (dentigerous cyst) can behave in extremely aggressive manner (1) . It is worth of mention that dentigerous cyst can not be diagnosed using radiographic evidence only but must be based on both macroscopic and microscopic examination of the specimen because various other lesions (such as unicystic ameloblastoma and odontogenic keratocyst) can occur in the position(2,3) .
The frequency of dentigerous cyst formation has been estimated to constitute 1.44 per 100 unerupted teeth (4) . Furthermore, the risk for individual teeth to develop dentigerous cyst varies considerably. In case of mandibular third molars, the frequency of impaction is roughly the same as that of cyst formation, whereas maxillary third molars have a much higher frequency of impaction than cyst involvement, suggestion that this tooth has a much lower relative risk of developing a dentigerous cyst than its mandibular counterpart(5) . Similarly the risk of cyst formation around the crowns of unerupted mandibular first premolars, maxillary incisors, or mandibular second molars is very high, although the frequency of failure of eruption of these teeth is extremely low (6) .
The aim of the present study is to find the incidence, clinico- pathological variation of dentigerous cyst in a review of series of dentigerous cyst from 1990-2000 such information are valuable to clinician as it help in the formulation of a working diagnosis and timing management decisions and approach to treatment.
Material and Methods
All cases of dentigerous cyst over the period between 1990- 2000 were recorded from the laboratory of Oral Pathology Departement, College of Dentistry, University of Baghdad.
The clinico-pathological details were taken from the archives file of the Department of Oral Pathology. All cases diagnosed histologically as dentigerous cyst were analyzed according to the age, sex, duration , site distribution, clinical presentation, radiographic appearance and histopathologic details based on the individual pathologic report of each case. These files more checked for adequacy of information given by surgeon regarding the cases at question.
Results
From the total 2410 oral biopsy, 235 cases were diagnosed as jaw bone cyst, thirty-seven cases were diagnosed as dentigerous cyst, accounting (15.7%) of all jaw bone cyst and (1.5%) over all oral surgical biopsies.
The age of the patients ranged from 5 to 50 years, with a peak incidence in the second decade of life, and the mean age was (22.2) years. The males were affected more than the females with a ratio of (1.5:1). ( Table 1) .
Regarding the site, (20 cases 54%) occurred in the maxilla and (17 cases 46%) in the mandible. In four cases the specific region was not recorded. However, for the maxilla, the most common affected site was canine region (15 cases = 40.5%). While for the mandible the most common affected site was molar region (7 cases = 18.9%), followed by canine region (4 cases = 10.8%)( table 2).
The duration of the symptoms ranged from one month to 4 years (median = 11 months). The initial presenting symptom (for all 37 patients) was intra-oral alveolar swelling, associated with pain in only 3 cases, parasthesia was noted in only one case. Moreover, one case was recorded as a recurrent case after 12 years.
The dentigerous cyst appears as circumscribed radiolucency associated with impacted tooth (Figure 1).
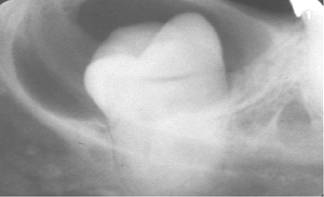
Fig1: Radiographic picture of Dentigerous cyst
The majority of the cysts show unilocular radiolucency (24 cases 80%) whereas 6 cases appear as multilocular. In the remainder 7 cases, the locularity were not recorded by the surgeon, in addition, 8 cases showed root resorption of the adjacent tooth. Moreover, odontom was associated with dentigerous cyst in only one case, and in two cases, the cyst was associated with supernumerary tooth in the upper incisor area.
All of the pathologic reports describe a similar histological picture (Figure 2).
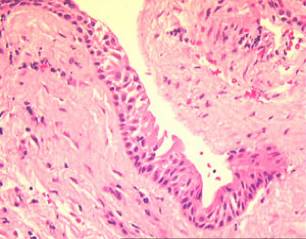
Fig 2: Histopathological picture of Dentigerous cyst
The lesions consist of a fibrous connective tissue wall which is loosely arranged. The epithelium lining consist of two to three layers of cubiodal epithelial cell. Four cases and due to infection the fibrous wall become more collagenized, with a variable infiltration of chronic inflammatory cell. In some areas hyperplastic squamous epithelial lining was seen especially in older patients. Moreover, characteristic ameloblastoma was seen in the wall of dentigerous cyst in a 25 years old female with about one year duration.
Table (1): Age&sex distribution of 37 cases of dentigerous cyst
Age group (years) |
Number |
Male |
Female |
Male:Female ratio |
0-10 |
9(24.3%) |
6(16.2%) |
3(8.1%) |
2:1 |
11-20 |
11(29.7%) |
6(16.2%) |
5(13.5%) |
1.2:1 |
21-30 |
7(18.9%) |
4(10.8%) |
3(8.1%) |
1.3:1 |
31-40 |
3(8.1%) |
2(5.4%) |
1(2.7%) |
2:1 |
41-50 |
7(18.9%) |
4(10.8%) |
4(10.8%) |
1.3:1 |
Total |
37(100%) |
22(59%) |
15(41%) |
1.5:1 |
Table (2): Site distribution of 37 cases of dentigerous cyst
Jaw |
Incisor |
Canine |
Premolar |
Molar |
Unknown |
Total |
Maxilla |
2(5.4%) |
15(40.5%) |
1(2.7%) |
0 |
2(5.4%) |
20(54%) |
Mandible |
1(2.7%) |
4(10.8%) |
3(8.1%) |
7(18.9%) |
2(5.4%) |
17(46%) |
Total |
3(8.1%) |
19(51%) |
4(10.8%) |
7(18.9%) |
4(10.8%) |
37(100%) |
Discussion
The developmental odontogenic cysts occur rarely in the jaw bones as compared to inflammatory cysts. However, the present study , revealed that the dentigerous cyst is one of the most common jaw bone cyst (15.7%), this finding is in agreement with that conducted by Mourshed(4) and Daley et al., (7) .
The lesion occurs most often in the second and third decades of life (8). This is in harmony with this result in which the majority of patients were young, 27 out of 37 patients being under the age of 30 years (72.7%). However, Brown (9) reported in a study conducted on 81 diagnosed dentigerous cysts a higher prevalence in the fifth decade of life.
The present investigation showed that males were affected more than the females. A similar result was reported by Browne (9) . The reason for this sex difference is unknown. However, Daley and Wysocki(8) suggested that it may be related to smaller jaw size in female patients and a grater tendency for prophylactic extraction of third molar.
Regarding the site, dentigerous cyst in our study occurs
predominantly or exclusively in the maxillary cuspid area. This finding confirmed by previous studies (6,10,11) . However, Main (2) , Angela and Mario (5) reported that the common site for dentigerous cyst was in the mandibular third molar area.
The dentigerous cyst is frequently well circumscribed unilocular radiolucency which is often associated with an unerupted tooth (4,12) . The cyst appears to have a greater tendency than other jaw bone cyst to induce root resorption of adjacent teeth. By comparison, root resorption due to keratocyst appears to be very rare(6,11) . This finding is supported by this series, in which the majority of the cases (80%) appear as unilocular radiolucency and (21.6%) showed root resorption of adjacent teeth. Moreover, Stanley et al., (13) suggest that a pericoronal radiolucency larger than 4mm in greatest with as assessed on a panoramic radiograph is considered as small dentigerous cyst, to differentiate between the normal dental follicles and a pathological change.
Clinically, dentigerous cyst occur most often as painless intra-oral alveolar swelling(5) ,sometime the cyst associated with pain(2) . Our finding is the same, in which the majority of cases were seen in advanced stages. Pain was reported less frequently; tooth mobility and displacement were occasionally observed. Recurrence of dentigerous cyst is rare (14) . In our study only one case was recurred within a period of 12 years after treatment.
The histological features of our dentigerous cyst are similar to those seen elsewhere (12) . Kim and Ellis (15) , showed that the dentigerous cyst may be lined by stratified squamous epithelium, especially in older patient. In their study, Stanley et al., (16) found
that all follicles of patients older than 26 years were lined by squamous epithelium rather than cubiodal to columnar cell or reduced enamel epithelium. This confirm by our finding in which the lining epithelium show squamous metaplasia in the older patient. Furthermore, the dentigerous cyst may give rise to a variety of tumors, notably ameloblastoma, squamous cell carcinoma, mucoepidermoid carcinoma, and rarely other tumors (14,17,18,19) . In our study, only one case shows ameloblastic characteristic in the lining epithelium of the cyst. Therefore, every case mimic radiographic appearance of a dentigerous cyst should be confirmed pathologically in order to exclude any other aggressive lesions.
References
1- Main DMG. Epithelial jaw cysts: 10 years of the WHO classification. J Oral Pathol 1985; 14: 1-7.
2- Main DMG. Epithelial jaw cysts: A clinicopathological reappraisal. Br J Oral Surg.1970; 8: 114-25.
3-Tie-Jun Li, Yun-Tang Wu, Shi-Feng Yu, Guang-Yan Yu. Unicystic Ameloblastoma: A Clinicopathologic Study of 33 Chinese Patients. American Journal of Surgical Pathology 2000; 24(10): 1385-1392
4- Mourshed F. A roentgeographic study of dentigerous cysts: incidence in a population sample. Oral Surg Oral Med Oral Pathol 1964; 18: 47-53.
5- Angela Benn, Mario Altini. Dentigerous cysts of inflammatory origin: A clinicopathologic study. Oral Surg Oral Med Oral Pathol 1996; 81: 203- 209.
6- Shear M. Cysts of the jaws: recent Advances. J Oral Pathol 1985; 14: 43-59
7- Daley TD, Wysocki GP, Pringle GA. The relative incidence of odontogenic tumors: Oral and jaw cysts in a Canadian population.
Oral Surg Oral Med Oral Pathol 1994; 77: 276-80.
8- Daley TD, Wysocki GP. The small dentigerous cysts: A diagnostic dilemma. Oral Surg Oral Med Oral Pathol 1995; 79: 77- 81.
9- Brown RM. Metaplasia and degeneration in odontogenic cysts in man. J Oral Pathol Med 1972; 145-58.
10- Brown RM. The pathogenesis of odontogenic cysts: a review. J Oral Pathol 1975; 4: 31
11- Struthers PJ, Shear M. Root resorption produced by the enlargement of ameloblastomas and cyst of the jaws. Int J Oral maxillofac Surg 1976; 5: 128.
12- Shafer WG, Hine MK, Levy BM. A text book of oral pathology. 4th ed. Philadelphia: WB Saunders, 1983; 260- 5.
13- Stanley HR, Alattar M, Collett WK, Stringfellow HR Tr, Spiegel EH. Pathological sequelae of “neglected” impacted third molars. J Oral Pathol Med 1988; 17: 113- 17.
14- Ismail IM, AL-Talabani NG. Calcifying epithelial odontogenic tumor associated with dentigerous cysts. Int J Oral maxillofac Surg 1986; 15: 108- 11.
15- Kim J, Allis GL. Dental follicular tissue: misinterpretation as odontogenic tumor. J Oral maxillofac Surg 1993; 51: 762- 7.
16- Stanley HR, Krogh H, Pannkuk E. Age changes in the epithelial component of follicles (dental sac) associated with impacted third molars.
Oral Surg Oral Med Oral Pathol 1965; 19: 128- 39.
17- Holmlund HA, Anneroth G, Lundquish G, Nordnram A. Ameloblastoma originating from odontogenic cysts. J Oral Pathol Med 1991;
20:318- 21.
18- Maxymiw WF, Wood RE. Carcinoma arising in a dentigerous cysts: a case report and review of the literature. J Oral maxillofac Surg 1991; 49: 639-
43.
19- Waldron CA, Koh ML. Central mucoepidermoid carcinoma of the jaws: report of four cases with analysis of the literature and discussion of the relationship to mucoepidermoid, sialodontogenic, and glandular odontogenic cysts. J Oral maxillofac Surg 1990; 48: 871- 7.
Click
on these links to visit our Journals:
Psychiatry
On-Line
Dentistry On-Line | Vet
On-Line | Chest Medicine
On-Line
GP
On-Line | Pharmacy
On-Line | Anaesthesia
On-Line | Medicine
On-Line
Family Medical
Practice On-Line
Home • Journals • Search • Rules for Authors • Submit a Paper • Sponsor us
All pages in this site copyright ©Priory Lodge Education Ltd 1994-


